What is your diagnosis?
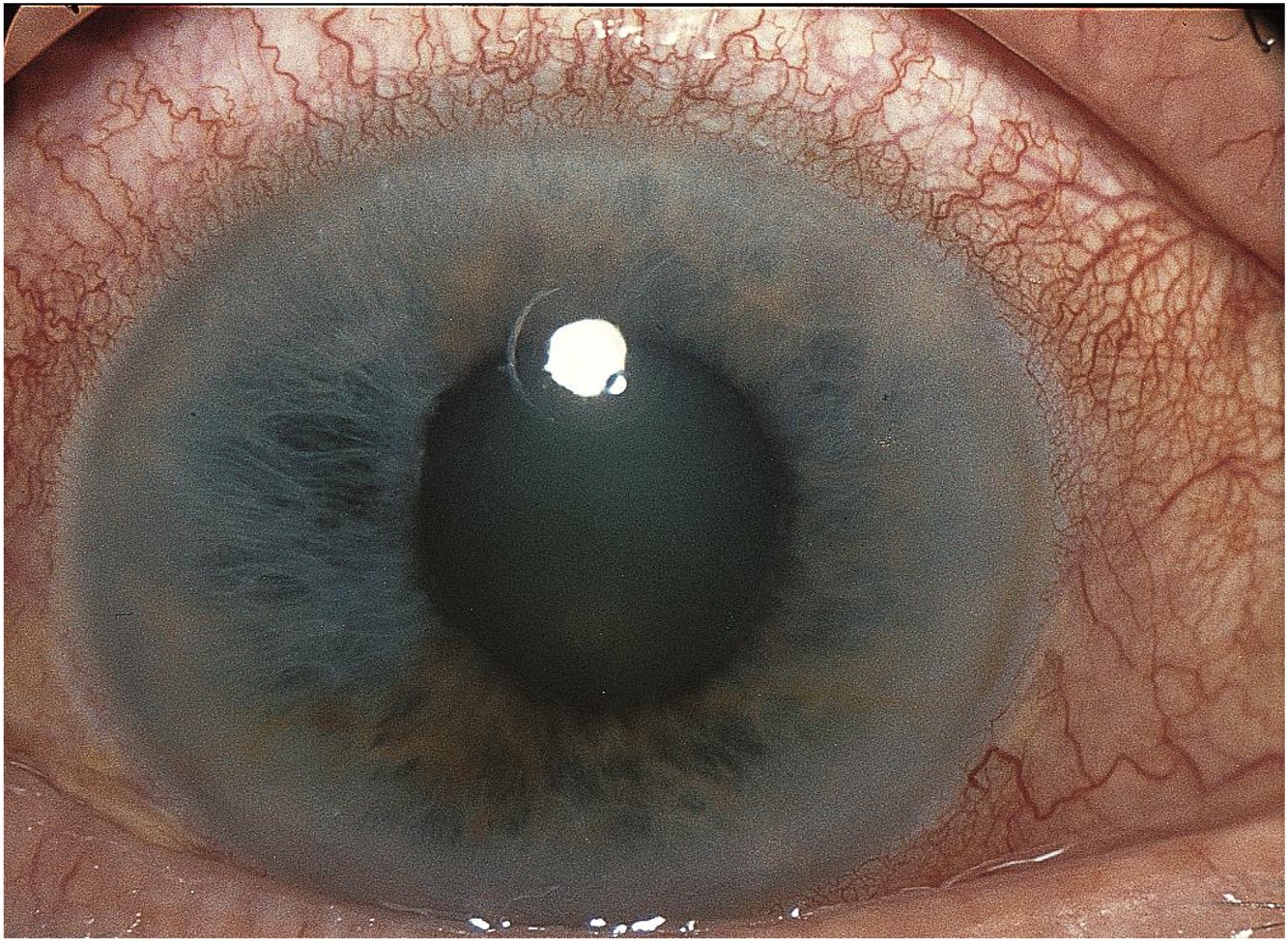
A 60-year-old woman presents with a newly painful, red right eye and blurred vision.
The diagnosis is...
![]()

The image is consistent with a diagnosis of acute angle-closure glaucoma (AACG):
- This rare but urgent condition is characterized by blurred vision, painful red eye, headache, nausea, and vomiting.
- AACG is caused by an abrupt increase in intraocular pressure (IOP)—typically above 40 mm Hg—due to total closure of the angle between the iris and the cornea, where fluid should usually drain out of the eye.
- The goal of treatment is to lower IOP, and the prognosis is favorable if pressure is controlled.
- AACG in one eye increases the risk of developing the condition in the other eye.
- Acute angle closure can occur in patients with preexisting chronic angle-closure glaucoma.
What is the role of the primary care or emergency medicine physician?
![]()
If AACG is suspected, the primary care physician or emergency physician should administer IOP-lowering medications and refer the patient to an ophthalmologist immediately to prevent damage to the optic nerve and vision. IOP-lowering medications include topical eye drops and oral or intravenous (IV) options, such as acetazolamide or mannitol.
Pain and nausea control should also be addressed.
What is the role of the ophthalmologist?
![]()
- Diagnose the condition via a slit-lamp exam and gonioscopy of the anterior chamber. Examination will show a narrow space between the iris and the cornea, the iris bowed forward, and often a thick, cataractous lens.
- Begin treatment to lower IOP.

What is the treatment?
![]()
The goal of treatment is to lower IOP and prevent or limit optic nerve damage. Initial treatments include topical eye drops (beta-blockers, alpha-2 agonists, and cholinergic agonists), oral or IV carbonic anhydrase inhibitors (acetazolamide), or IV hyperosmotic agents (mannitol).
If IOP does not respond to the above treatments, laser peripheral iridotomy is performed to create a route for fluid from the area that produces fluid to the area that drains it. After resolution of an acute attack, laser peripheral iridotomy of the other eye and cataract extraction should also be considered.

Learn more: Ophthalmology resources for medical students
![]()